
Key points
- Inaccurate injury data hinders prevention initiatives.
- BLS data comes from employer records, which may be inaccurate due to workers hiding injuries or employers lacking proper recordkeeping knowledge, according to one source.
- A solution for gathering more accurate data – either from using alternative sources or through OSHA collection initiatives – has support but comes with its own drawbacks.
What is the state of safety?
It’s a question Safety+Health explores every year by speaking with experts and looking at the most recent data.
The largest national source of occupational injury and illness data comes from the Bureau of Labor Statistics’ annual Survey of Occupational Injuries and Illnesses. This survey provides an estimate of nonfatal injuries nationwide, allowing stakeholders to get a clearer picture of workplace safety in the United States.
Accurate data leads to a better understanding of injuries and illnesses, and plays a key role in regulatory, enforcement and research decisions. But data gathered from inaccurate recordkeeping that underreports or undercounts injuries and illnesses can have repercussions.
“Underreporting obscures reality and misleads all the key stakeholders when issues of work and health are discussed,” states a commentary published in a special issue of the American Journal of Industrial Medicine (Vol. 57, No. 10).
Underreporting is occurring. Several studies conducted over the past few years – including those published in the journal’s special issue – have concluded that the SOII undercounts the number of workplace injuries and illnesses occurring throughout the country.
The problem
The full extent of the problem is unknown – no studies have examined injury and illness undercounting on a national scale. However, Ken Kolosh, statistics department manager at the National Safety Council, said research has been conducted at the state level, and stakeholders can use the data to conclude that a “significant” undercounting issue exists nationwide.
The issue needs to be addressed, according to Les Boden, a professor of environmental health at Boston University’s School of Public Health, who contributed to studies published in the special issue of AJIM.
“If injuries and illnesses are undercounted by as much as 50 or 60 percent, then they appear to be less of a problem than they really are,” Boden said.
The AJIM commentary was authored by Emily Spieler, Edwin W. Hadley Professor of Law at Northeastern University School of Law in Boston; and Gregory Wagner, a senior advisor at NIOSH. It lists consequences of inaccurate or underreported injury data, including:
- An inability for state and federal agencies to evaluate risks and develop effective enforcement initiatives
- Diminished appreciation for the economic toll of injuries
- Misdirected occupational safety and health research
- Reduced pressure on employers, health agencies and legislators to lower exposure to occupational health hazards
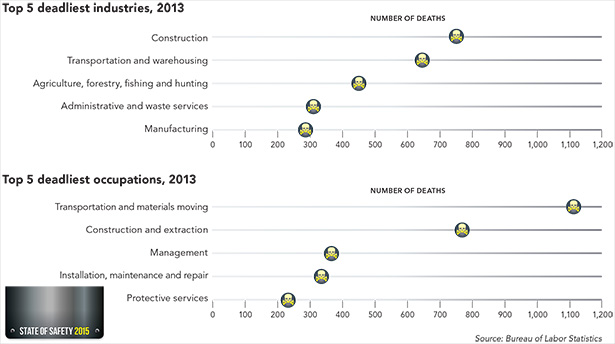
In 2013, 4,405 workers were killed on the job, according to preliminary data released in September by the Bureau of Labor Statistics.
This is a decline from the 2012 final fatal work injury count of 4,628. The number of deaths per 100,000 full-time equivalent workers also fell between 2012 and 2013, with 3.2 deaths occurring in 2013 compared with a rate of 3.4 the previous year.
Final workplace fatality counts typically increase by about 165 cases from the preliminary count. If this year’s preliminary figure conforms to the average, the fatal worker injury total will still fall below the 2012 total, continuing the ongoing trend of declining injuries. Final 2013 fatality data is expected in early 2015.
Fatalities did not decrease uniformly, however. Fatal work injuries rose 7 percent among Hispanic or Latino workers – the only racial or ethnic group whose fatal work injuries increased from 2012 to 2013. Two-thirds of these deaths involved foreign-born workers. Of the 845 total fatal work injuries involving foreign-born workers, nearly half were born in Mexico. “We need to find better ways to protect foreign-born workers,” said Ken Kolosh, statistics department manager at the National Safety Council.
The source
Inaccurate data is the result of a number of issues. For starters, BLS data comes from employers, who have to be aware of an injury before it can be recorded. Information about a worker injury that occurred offsite or on a different shift may never make it back to the individuals responsible for recordkeeping.
Employees also may choose not to report an injury. Workers’ compensation laws passed in the past 20 years have made it difficult in some states for injured employees to apply for and receive benefits. As a result, Boden said, workers have less incentive to report injuries.
Employment stability is a factor, too. Fewer workers have long-term, secure jobs. The less job security an individual has, the more he or she might worry that reporting an injury may threaten his or her employment, Boden claims.
In a study published in the special issue of AJIM, researchers found that 90 percent of employers in Washington state did not comply with OSHA recordkeeping regulations, which could directly contribute to BLS undercounting injuries.
Sara Wuellner, co-author of the study, is an epidemiologist for the Safety and Health Assessment and Research for Prevention Program at the Washington State Department of Labor and Industries. She said employers may not comply with recordkeeping requirements for a number of reasons.
For instance, employers may lack proper education on the requirements, or previously had been given inaccurate information. Maybe they received recordkeeping training decades ago, and need a refresher course. Or perhaps they simply did not know about the requirements in the first place. “People in certain industries or certain employers make the effort to educate themselves,” Wuellner said. “But that seems to be a small portion.”
Photo credits: Yuliyan Velchev/iStock/Thinkstock; outer diamond images (clockwise from top): Emily Lai/Hemera/Thinkstock; eric1513/iStock/Thinkstock; Patrick Heagney/Getty Images; aerogondo/iStock/Thinkstock; thavornc/iStock/Thinkstock; Bureau of Labor Statistics; Christian Lagereek/iStock/Thinkstock; manfredxy/iStock/Thinkstock; center image: phil morley/iStock/Thinkstock
OSHA’s new rule
More routine reporting of injury and illness records could help improve data accuracy, Wuellner said. If employers report their records to the government more frequently, she said, recordkeeping requirements might have a stronger presence in the workplace.
The Improve Tracking of Workplace Injuries and Illnesses rule – an OSHA rule in the works as of press time – would require certain employers to submit their annual injury summary to the agency each year. Employers who keep records and have more than 250 workers would have to submit injury reports on a quarterly basis. (See More data, more problems? Safety+Health, December 2014.)
Under the proposed rule, OSHA would collect injury reports from about 440,000 establishments – more than double the amount that currently receives the annual BLS survey.
“OSHA could collect data from many more employers and potentially, in that case, be able to see things that the BLS isn’t able to see in its data,” Boden said.
Or maybe not. Because OSHA’s proposed rule relies on employers to collect injury information, many problems associated with undercounting could still exist.
Some stakeholders believe that employers are not always truthful about injury data, as it may be used for a variety of business practices such as winning contractor bids or internal financial awards.
“People are uncomfortable with the idea that the reporting is being done by the employer, so there will always be a suspicion of ‘Are they hiding something?’” Wuellner said.
Workers’ compensation
Some stakeholders have suggested that using non-employer-provided information could improve the accuracy of injury data. This has been done before. In the 1980s and early ’90s, BLS and state-based researchers found that 50 percent of all occupational fatalities were not being reported. For example, in 1990, BLS estimated only 2,900 work-related fatalities. In contrast, the National Safety Council estimated more than 10,000, and NIOSH estimated about 5,700 in 1989. This led to BLS revising how it counted fatalities by looking at multiple sources, according to Boden.
One suggestion for supplementing the current BLS survey is to use workers’ compensation data. Although not all workplace injuries could be captured using this data, those that may fall through the cracks in one system might be caught by another.
But using multiple data sources can have drawbacks as well. Matching the data sets to ensure injuries are not double-counted is laborious, Kolosh said. The process would take longer and be more costly, resulting in a delay in when the data is published. (BLS currently releases its injury data for any given year near the end of the following year.)
“If I was anxious to benchmark my performance with national averages, I would want those benchmarks as soon as feasibly possible,” Kolosh said.
Further complicating matters is the lack of uniformity. Workers’ compensation is handled by individual states, and every state operates differently.
Wuellner said a combination of two systems might be a solution: Employers may receive timely SOII data for a national picture, but more detailed information from multiple sources could come later.
Even in this scenario, workers’ comp data is still not easily comparable from state to state, Wuellner said. Safety prevention efforts relying on workers’ comp data would have to come from within each state, requiring individual states to know and understand their data sources, as well as have the resources to implement prevention efforts, she noted.
Illnesses: An even larger issue?
Is the undercounting of occupational illnesses even more severe than that of injuries?
Illnesses account for only 10 percent of all nonfatal cases identified by the Bureau of Labor Statistics. This ratio does not match up with occupational disease-related fatalities, which some estimates show greatly outnumber deaths due to occupational injuries, according to a commentary published in a special issue of the American Journal of Industrial Medicine (Vol. 57, No. 10).
The commentary even said the title of the BLS survey used to gather data – the Survey of Occupational Injuries and Illnesses – is a misnomer because of the very low estimate of occupational illnesses captured. However, other sources, such as workers’ compensation data, are equally poor at estimating occupational illnesses, said Les Boden, a professor of environmental health at Boston University’s School of Public Health.
“It’s generally accepted that BLS and workers’ compensation data are of virtually no use in surveillance of chronic occupational diseases,” Boden said.
The SOII has trouble tracking occupational illnesses primarily because of the long period of time in which diseases develop, according to the commentary. The survey is designed to capture immediate, acute incidents that are easily identifiable as work-related – which is the case with many injuries.
Further, employers and health care providers may not recognize an employee’s disease as work-related.
Steps are being taken to resolve the matter and get a more accurate count of occupational-related illnesses. The Office of the National Coordinator for Health Information Technology is encouraging health care providers to adopt interoperable electronic health records. Doing so would allow better sharing of vital information that could lead to improved treatment for ill workers.
Meanwhile, NIOSH is working with various organizations to develop standards to ensure employees’ occupational information is included in data collected by the electronic records. This could help doctors determine whether a chronic illness is related to workplace exposures.
Health care providers would need a lot of training to ensure the relevant occupational information is included in the electronic health record, but the result could be a more accurate occupational illness count, according to Ken Kolosh, statistics department manager at the National Safety Council.
“If physicians could start tracking work-relatedness in medical records, that could go a long way to start identifying the true impact of occupational illnesses,” Kolosh said.
Still a value
Despite these issues, the BLS survey data has value. Boden pointed out that the data can highlight the biggest worker safety issues, alerting safety professionals and researchers to the types of injuries occurring, as well as growing developments.
“If I’m an employer, then I want to find out quickly that there’s some emerging problem in the workplace,” Boden said. Whether that problem results in 100 cases or 200 cases is not as important as knowing about the problem in the first place, he said.
The overall trend of declining injuries is likely to be accurate, too, according to Kolosh, as it mirrors declining fatality figures. The undercounting of injuries also is likely to be uniform, suggesting the proportions of individual types or causes of injuries would remain unchanged by more accurate data, Boden said.
Even so, many stakeholders agree that the undercounting of BLS data is a problem, and more accurate data is necessary.
“Ultimately, if the goal is to prevent injuries in the workplace, that occupational injury data is crucial,” Wuellner said.
The Bureau of Labor Statistics delayed the release of 2013 nonfatal occupational injury and illness data, which at press time was not fully available. The delay stemmed from data processing errors unrelated to the undercounting problem explored in this article.
Read about updates on nonfatal data from BLS.

